By Charles A. Pilcher MD FACEP
November, 2015
What are the first things an emergency physician should think of when confronted with a patient complaining of new onset chest pain?
Heart attack? Sure. But given how common heart attacks are and how attuned to that diagnosis most physicians are (or should be), how often does a physician actually fail to consider an acute MI as the cause?
Not very, I contend. Yes, there may be a lot of malpractice lawsuits over missed MI’s, but on a percentage basis, it’s far less than one would expect. Docs are generally quite good at diagnosing an MI, partly because MI’s are so common. Approximately 1.5 million heart attacks occur in the US each year for a frequency of about 6000 cases per 1,000,000 population. So an average community emergency department will see approximately one acute MI every day.
On the other hand, aortic dissection is rare, with approximately 2000 cases admitted to hospitals each year in the US and a frequency of 5-30 cases per million people per year. Thus, a busy ED might see only one case every year. That means that there are between 200 and 1200 acute MI’s for every aortic dissection.
A 2010 study by Brown et al. in the Society for Academic Emergency Medicine analyzed the frequency of malpractice claims for a variety of diagnoses. The top ten are shown below:
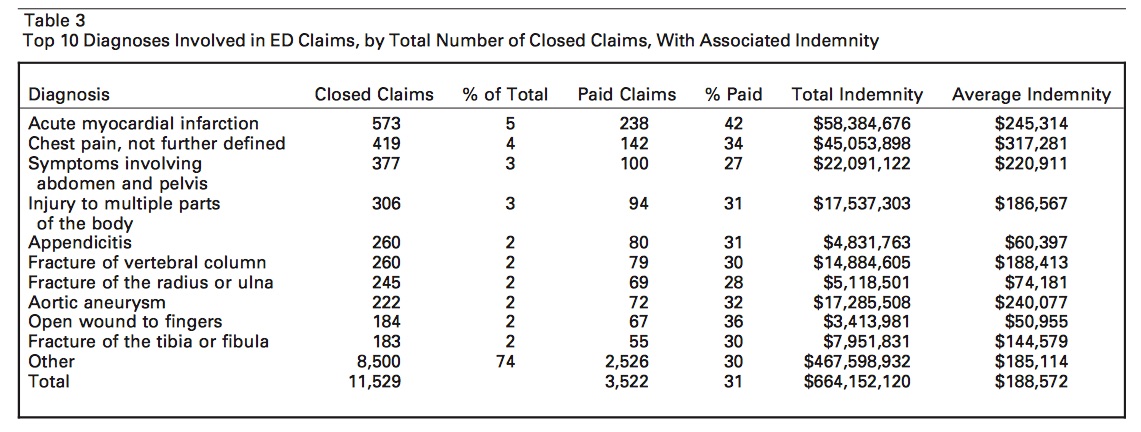
Note that every condition listed above is a common presentation in the ED – except one: Aortic aneurysm. Also note that there were only 573 lawsuits related to acute MI. Yet there were 222 lawsuits related to aortic aneurysm. Given the rarity of the latter condition, this is a huge percentage of cases resulting in litigation.
Using the above data, let’s accept that an MI is 500 times more common than an aortic dissection. Then note that there are only about 2.5 times as many lawsuits related to MI than are related to aortic aneurysm. A rough extrapolation of this data thus indicates that a lawsuit is filed in about 200 times as many cases of aortic aneurysm/dissection as are filed in cases of MI.
My experience as an expert witness bears this out. Lawsuits for missed aortic dissection are frequent. Lawsuits for missed MI are rare.
Why is this so?
Returning to the opening sentence of this Perspective, “What are the first things an emergency physician should think of when confronted with a patient complaining of new onset chest pain?
They are those things that can kill a patient if an ED doc does not consider them in his/her differential and rule them out – either with a well-documented history and exam or with appropriate testing. The top 3 are:
- Pulmonary embolus
- Acute coronary syndrome without MI
- Aortic dissection
Often the frequency of a condition lulls us into a sense of complacency. We readily think of the easy diagnosis, the common diagnosis, and if that is ruled out – EKG normal, d-dimer normal, cardiac enzymes normal – we feel safe sending a patient home. But if we don’t rule out the aortic dissection, the pulmonary embolus and/or the acute coronary syndrome with normal lab and EKG, that patient could be dead in a matter of hours. In fact, according to a study by Kurabayashi et al. in 2011, the diagnosis of aortic dissection is missed in approximately 1 of every 6 presentations, frequently in patients able to walk into the ED.
Thus, the key to making the diagnosis is to think first not of acute MI when seeing a patient with chest pain, but to think – first of the those serious but rare conditions that, if missed, could result in a dead patient and years as a defendant in a malpractice lawsuit. One must then document the process by which those conditions were ruled out. Once considered, all of the top 3 diagnoses associated with chest pain can be easily ruled in or out, resulting in greater patient survival and more physician heroes in the ED.